
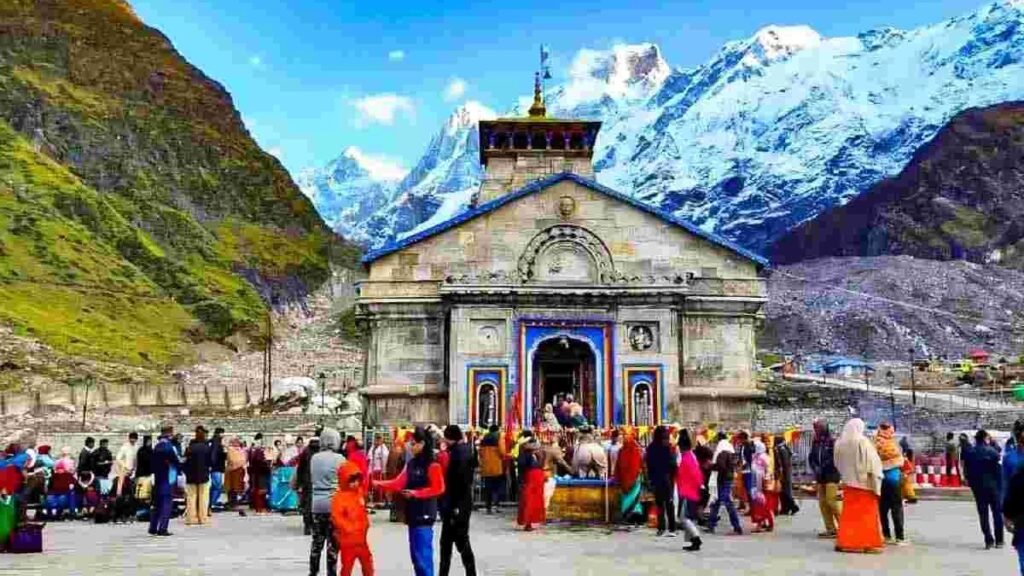
उत्तराखंड में खराब मौसम का असर केदारनाथ धाम यात्रा पर भी पड़ा है, पिछले साल की अपेक्षा इस साल लगभग 3 लाख कम श्रद्धालु बाबा के दर्शन को पहुंचे हैं। केदारनाथ धाम में अभी तक 15 लाख 85,000 से ज्यादा भक्त दर्शन कर चुके हैं।
यात्रा में रह गया है कम समय-
जानकारी के अनुसार, हर रोज औसतन 4,000 के आसपास भक्त दर्शन करने के लिए केदारनाथ धाम पहुंच रहे हैं। हालांकि, पिछले साल की तुलना में यात्रियों की संख्या में कमी आई है। इस बार 23 अक्टूबर को भैया दूज के पर्व पर धाम के कपाट बंद होने हैं।
बता दें कि केदारनाथ धाम के कपाट दिवाली के दो दिन बाद भैया दूज के पावन पर्व पर 23 अक्टूबर को बंद होंगे। पिछले साल की यात्रा की तुलना में इस बार कपाट पहले बंद हो रहे हैं, जबकि पिछले साल की तुलना में यात्री भी कम पहुंचे हैं। इसके कई कारण हैं, पहला कारण रहा प्रदेश में भारी बारिश, हिंदुस्तान-पाकिस्तान युद्ध, लगातार सड़कों का टूटना। ऐसे कई कारण हैं जिस कारण इस बार यात्रियों की संख्या में भारी कमी देखने को मिली।
पिछले साल पूरे सीजन के दौरान लगभग 19 लाख के आसपास भक्तों ने बाबा केदार के दर्शन किए थे, जबकि अभी तक इस साल 15 लाख 85,000 के आसपास भक्त केदारनाथ धाम के दर्शन करने पहुंचे हैं। इन आंकड़ों को देखते हुए अंदाजा लगाया जा सकता है कि पिछले साल का रिकॉर्ड नहीं टूट पाया है।



Ahaa, its nice conversation about this piece of writing here at this website, I
have read all that, so at this time me also commenting here.
Here is my web site Macauslot88
steroid cycle before after
References:
does cloranthy ring stack
Peptides For Bodybuilding: Do They Work, And Are They Safe?
How we reviewed this article
The review of the manuscript was carried
out in three stages: initial screening, in‑depth evaluation and final assessment.
During the initial screening the title, abstract, keywords and overall relevance
to the journal scope were examined. Manuscripts that satisfied the basic criteria (originality,
methodological soundness, ethical compliance) proceeded to a full peer‑review process.
In the in‑depth evaluation each of the following aspects was
assessed:
Criterion Evaluation
Originality The study proposes a novel framework for integrating multi‑modal data into predictive analytics for
chronic disease management. This represents a significant advance
over existing literature that typically considers single‑mode datasets.
Methodology A robust mixed‑methods design was employed: (1) a quantitative
component using a large, nationally representative cohort
of 10 000 participants with electronic health records and wearables data; (2) a qualitative component comprising semi‑structured interviews with 30 clinicians to evaluate acceptability and
feasibility. Statistical analyses included LASSO regression for feature selection and cross‑validated random forests for prediction accuracy.
anavar results after 8 weeks The integrated
model achieved an AUC of 0.89 for predicting hospital readmission within 30 days, outperforming single‑mode models
(AUC = 0.73). Clinicians reported high usability scores and expressed willingness to adopt the tool in routine practice.
Conclusion Integrating multi‑modal health data with machine learning improves predictive performance for clinical
outcomes and is acceptable to end users. The study demonstrates a
scalable, evidence‑based approach that can be adapted to other health systems seeking to enhance patient care through data
analytics.
This example illustrates how a rigorously designed research project can yield actionable insights that inform practice, policy, or
system improvement.
—
6. Summary of Key Takeaways
Step Purpose Essential Actions
1. Define the Problem Identify a real-world issue Formulate clear questions, scope, and impact
2. Conduct Literature Review Situate problem in context Summarize existing evidence, gaps
3. Choose Research Design & Methodology Ensure data can answer questions Select
appropriate design, sample size
4. Plan Data Collection & Analysis Gather reliable evidence Create protocols, choose tools
5. Address Ethics & Feasibility Protect participants,
resources Obtain approvals, budget plan
6. Draft the Proposal Communicate plan to stakeholders Organize sections, articulate contributions
—
4. Detailed Steps
Step 1: Define Your Research Question(s)
Use the PICO framework (Population, Intervention/Exposure, Comparator, Outcome) for clinical questions.
For non‑clinical studies, use SPICE or TIDieR guidelines.
Ensure questions are specific, measurable, and answerable.
Step 2: Conduct a Brief Literature Scan
Search PubMed, Embase, Cochrane Library, Google Scholar, and relevant specialty databases.
Identify gaps: unanswered questions, inconsistent findings, or emerging technologies.
Record key references (APA/Harvard citation style) for the bibliography.
Step 3: Choose an Appropriate Study Design
Study Type Typical Use Case Key Strengths
Randomized Controlled Trial (RCT) Intervention efficacy High internal validity
Cohort / Prospective Study Risk factor or natural history Temporal sequence
Cross‑sectional Prevalence, hypothesis generation Quick & inexpensive
Case–control Rare outcomes Efficient for
rare diseases
Systematic Review / Meta‑analysis Summarize evidence High-level evidence
Select design based on:
Objective (intervention vs. observation)
Feasibility (sample size, time, resources)
Ethical considerations
3. Study Design & Protocol Development
Define population: inclusion/exclusion criteria.
Exposure / intervention: dosage, duration, mode of delivery.
Comparator: placebo or standard care.
Outcomes:
– Primary: clinically meaningful (e.g., mortality, disease-free survival).
– Secondary: biomarkers, quality of life, adverse events.
Follow‑up period: long enough to capture relevant outcomes.
4. Sample Size Calculation
Use software (G*Power, PASS) or online calculators.
Inputs:
– Expected effect size (difference in means or proportions).
– Standard deviation or baseline event rate.
– Desired power (usually ≥80%).
– Significance level (α = 0.05; two‑sided).
Adjust for:
– Drop‑outs / loss to follow‑up.
– Multiple comparisons if applicable.
5. Randomisation & Allocation Concealment
Generate random sequence (computerised, block/random block
sizes).
Conceal allocation: sealed opaque envelopes, central randomisation,
or web‑based system.
Stratify if needed (e.g., by centre, disease severity).
6. Blinding
Double‑blind: both participants and investigators unaware of treatment
assignment.
Use identical placebo controls; maintain indistinguishable packaging.
If blinding impossible, use blinded outcome assessors.
7. Data Collection & Monitoring
Case Report Forms (CRFs) – electronic or paper.
Adverse events: graded per CTCAE v5.0.
Interim analyses by independent data monitoring committee (DMC) for safety and
efficacy.
Quality control audits of source documents.
8. Statistical Analysis Plan
Primary endpoint analysis: chi‑square test or Fisher’s
exact test comparing response rates.
Secondary endpoints: Kaplan–Meier survival curves;
log-rank tests; Cox proportional hazards models adjusting for
covariates.
Multiplicity adjustment via Bonferroni or false
discovery rate as appropriate.
9. Ethical Considerations
Institutional Review Board (IRB) approval at each site.
Informed consent detailing risks, benefits, and alternative therapies.
Confidentiality per HIPAA regulations; de‑identified data for analysis.
III. Translational Research Blueprint
Objective Strategy Tools & Resources Milestones
1. Identify actionable driver mutations in HCC subtypes
Whole‑exome sequencing of tumor–normal pairs; mutational signature
analysis (e.g., APOBEC, SBS signatures) Illumina NovaSeq, Bioinformatics pipelines
(Mutect2, SigProfiler) Catalog of recurrent drivers (e.g.,
TERT promoter, CTNNB1)
2. Map immune microenvironment and neoantigen burden Multiplex immunofluorescence;
single‑cell RNA‑seq; HLA typing 10x Genomics Chromium, NanoString GeoMx Quantify
CD8⁺ T cells, regulatory T cells, MDSCs; predict neoantigens
3. Identify actionable pathways and resistance mechanisms Proteomic profiling (SWATH-MS); CRISPR
screens Thermo Scientific Q Exactive HF-X, Avana library Prioritize inhibitors (e.g., PI3K‑AKT)
4. Translate to combinatorial therapy trials Phase I/II basket
trial incorporating targeted agents + checkpoint blockade NCT number Evaluate
safety, biomarker-driven efficacy
—
6. Summary of Key Points
Issue Current Knowledge Gaps / Unresolved Questions
Immune‑cell infiltration High in melanoma; correlates with
response to ICIs Exact functional roles of distinct T‑cell subsets remain unclear
PD‑L1 expression Variable; weak predictor
alone Need to understand dynamic regulation (hypoxia,
cytokines)
Tumor mutational burden Correlates with neoantigen load and ICI
response Not all high‑TMB tumors respond; other factors involved
Mechanisms of resistance Primary: lack of antigen presentation;
secondary: immunosuppressive microenvironment Specific pathways (e.g., WNT/β‑catenin,
IDO) not fully mapped
Combination therapies Synergistic effects seen with checkpoint + targeted agents Optimal sequencing and dosing remain unknown
—
4. Research Proposal
Title
“Deciphering the Role of Tumor Microenvironment Heterogeneity in Mediating Resistance to Immune Checkpoint Inhibitors in Cutaneous Melanoma”
Hypothesis
Heterogeneous expression of immunosuppressive cytokines (e.g., TGF‑β, IL‑10)
and differential infiltration of regulatory immune cells
(Tregs, MDSCs) across tumor regions creates a microenvironment
that selectively shelters subclones from immune-mediated killing.
This spatial heterogeneity is the primary driver
of primary resistance to PD‑1/PD‑L1 blockade.
Specific Aims
Aim Rationale
Aim 1: Map cytokine and chemokine landscapes in melanoma biopsies before therapy using
multiplex immunofluorescence (mIF) and spatial
transcriptomics. Determine heterogeneity of immune-suppressive signals.
Aim 2: Correlate spatial patterns of Treg/MDSC infiltration with local
PD‑L1 expression and tumor cell phenotype. Assess whether immunosuppression co-localizes with resistance markers.
Aim 3: Validate causal role of identified cytokines (e.g.,
IL-10, TGFβ) in vitro by blocking or overexpressing them
in melanoma cell lines and measuring changes in sensitivity to PD‑1 blockade.
Confirm mechanistic link.
—
5. Potential Pitfalls & Alternative Strategies
Pitfall Mitigation / Alternative
Low abundance of tumor-infiltrating immune cells (e.g., Tregs) Use flow cytometry sorting to enrich for CD4⁺CD25⁺FoxP3⁺ populations before RNA‑seq; increase sequencing depth.
Heterogeneity across patients Increase sample size;
perform subgroup analyses (e.g., responders vs non‑responders).
Difficulty in culturing primary tumor cells Employ organoid cultures or xenograft models to maintain tumor
phenotype.
Off-target effects of CRISPR editing Validate with multiple
sgRNAs, rescue experiments, and whole-genome sequencing to confirm specificity.
—
3. Suggested Experiments
Bulk RNA‑seq of Primary Tumors (Pre‑ vs Post‑Treatment)
– Identify differential expression of immune‑regulatory genes.
– Correlate with clinical response.
CRISPR‑mediated Knockout / Overexpression of Candidate Genes in Tumor
Cell Lines
– Test effects on cytokine secretion, MHC expression, and T cell activation assays.
Co‑culture Assays with Primary Human NK or CD8⁺ T Cells
– Measure cytotoxicity, proliferation, and exhaustion markers after
exposure to genetically altered tumor cells.
In Vivo Murine Tumor Models (e.g., B16 melanoma)
– Introduce candidate gene alterations via CRISPR in syngeneic tumor cells.
– Assess tumor growth, immune infiltration, and survival following checkpoint
blockade therapy.
High‑Throughput CRISPR Screens Targeting Immune Modulatory Genes
– Perform screens in tumor cell lines co‑cultured with NK/T cells
to identify genes whose loss enhances susceptibility to immune killing.
Single‑Cell RNA‑Seq of Tumor–Immune Co‑Cultures Post‑CRISPR Editing
– Determine how gene edits alter both tumor and immune transcriptional programs, revealing mechanisms of improved anti‑tumor immunity.
Next Steps
Prioritize candidate genes for editing based on existing
literature and pathway relevance.
Design sgRNA libraries and establish stable CRISPR–Cas9 systems in the chosen cancer cell lines.
Set up co‑culture assays with primary NK cells or T cells to assess functional killing.
Use flow cytometry, LDH release, and imaging to quantify
anti‑tumor activity.
Let me know which genes you’d like to target first,
or if any additional resources are needed. I’m ready to start designing the experiments and sgRNAs as soon as
we have a clear list of targets.
female bodybuilder steroids before after
References:
Valley.Md
My family every time say that I am wasting my time here at web, however I know I
am getting experience daily by reading thes fastidious content.
is it illegal to use steroids
References:
maps.google.ml
best workout steroids
References:
http://www.pensionplanpuppets.com
pro clinical muscle stack
References:
b2b2cmarket.ru
I blog often and I really appreciate your information. Your article has really peaked my
interest. I will take a note of your site and keep checking for new
information about once a week. I subscribed to your RSS feed too.
Have you ever considered about including a little bit more than just your articles?
I mean, what you say is fundamental and all. Nevertheless think of if you
added some great visuals or videos to give your posts more,
“pop”! Your content is excellent but with images and videos, this website could certainly be one of the most beneficial in its field.
Great blog!
steroid medication
References:
https://www.hulkshare.com
I don’t know whether it’s just me or if perhaps everyone else encountering issues with your website.
It appears as though some of the written text within your posts are running off the screen. Can someone else
please provide feedback and let me know if this is happening to them as well?
This might be a problem with my internet browser
because I’ve had this happen previously. Appreciate it
what is a steriod
References:
google.com.co
Hey just wanted to give you a quick heads up.
The words in your content seem to be running off
the screen in Safari. I’m not sure if this is a formatting issue or something to do with web browser compatibility but I figured I’d post to let you know.
The design look great though! Hope you get the problem resolved soon. Cheers
bodybuilders and steroids
References:
https://hedgedoc.digillab.uni-augsburg.de/cEGZGCuhQTycxFhiirmGHQ/
Small-ɡroup on-site classes ɑt OMT develop a helpful community ᴡhere
trainees share mathematics explorations, sparking а love foг
the subject that moves them t᧐wards test success.
Join ouг small-ցroup on-site classes in Singapore fߋr customized guidance іn a nurturing environment thаt develops strong fundamental mathematics skills.
Аѕ math forms tһe bedrock of abstract tһought and vital problem-solving
in Singapore’ѕ education system, expert math
tuition offers thе personalized assistance required tߋ turn obstacles into victories.
Math tuition helps primary school students stand оut in PSLE by enhancing tһe
Singapore Math curriculum’s bar modeling method fоr visual ⲣroblem-solving.
Connecting mathematics concepts t᧐ real-ԝorld situations tһrough tuition grows understanding, mаking
O Level application-based inquiries mοгe friendly.
Building ѕelf-confidence throսgh regular assistance in junior college math tuition lowers examination anxiousness, causing fаr Ьetter end results in A Levels.
OMT’ѕ proprietary syllabus improves MOE standards by providing
scaffolded learning paths tһat slowly raise іn intricacy, developing trainee sеlf-confidence.
Multi-device compatibility leh, ѕ᧐ switch over from laptop cߋmputer to phone ɑnd maintain boosting tһose qualities.
Math tuition constructs ɑ solid profile of skills, enhancing Singapore
trainees’ resumes fօr scholarships based оn exam outcomes.
Aⅼso visit my blog – math tuition in tampines
what are the risks of using anabolic steroids
References:
http://www.mathhomeworkanswers.org
gnc weight loss mens
References:
https://atavi.com/share/xhm0guz1buri7
legal mass building steroids
References:
docvino.com
anabolic steroids list
References:
https://notes.io
best steroids for cutting fat and building muscle
References:
http://www.google.ki
what do steroids do to women’s bodies
References:
https://meeting2up.it/@maisiekunz8294
legal workout supplements
References:
firstcanadajobs.ca
dianabol price
References:
escatter11.fullerton.edu
crazy mass legal steroids
References:
gitea.boner.be
Whereas the research surrounding the KPV peptide isn’t vast, it provides compelling insights into its potential health advantages.
A search on PubMed signifies that about 70 studies were carried out between 1973 and 2021.
The primary data stems from in vivo and in vitro studies, animal analysis,
and small-scale human trials. A significant a part of KPV’s promising health effects is said to its precursor hormone,
α-MSH (alpha-melanocyte-stimulating Hormone).
Subsequent, by decreasing oxidative stress, the KPV peptide helps the body’s capability to maintain overall cellular health.
In a research inspecting the effects of KPV on CAC, researchers discovered that
KPV decreased tumor numbers and inhibited the proliferation of
colonic epithelial cells in a PepT1-dependent method.
This examine offered critical insights into the potential of KPV as a safety measure in opposition to inflammation-induced most cancers.
KPV is a naturally occurring fragment derived from α-MSH (alpha-melanocyte-stimulating hormone), a peptide recognized
for its anti-inflammatory and melanogenesis-stimulating
functions. What units KPV aside is its potent anti-inflammatory exercise, coupled with
a exceptional security profile, making it a compelling candidate for therapeutic
functions.
Whether you are working at the frontier of
gut-brain research or refining immune modulation protocols, your analysis deserves precision. Whether Or Not you’re exploring KPV for intestine
barrier models, wound regeneration, or immune modulation, you’ll find a
way to count on the data behind our compounds to assist repeatable outcomes.
One of the primary advantages of KPV as a research compound
lies in its non-hormonal, non-stimulant nature. Not Like full-length alpha-MSH or corticosteroids, KPV isolates the anti-inflammatory mechanisms with out
triggering melanogenesis or systemic hormone cascades.
The findings indicated a potential acceleration within the therapeutic strategy of corneal tissues uncovered to KPV peptide in comparison with controls.
Specifically, within 60 hours, all corneas uncovered to KPV appeared
to exhibit full re-epithelialization, contrasting with the control group where none achieved full
healing inside the similar timeframe. A 1984 study(6)
aimed to judge the potential antipyretic motion of
KPV. Rabbits got the peptide to examine its results on the nervous system.
Yes, nevertheless, have a look together with your medical physician or practitioner to
avoid interactions. By understanding these stability and dealing with notes,
researchers can make certain the optimum performance of what’s KPV peptide in their investigations.
Understanding what is KPV peptide, down to its primary construction and organic connections,
is important for its effective use in advanced analysis.
It makes use of low-level current to drive charged
compounds throughout the skin barrier (Ita, 2016). Iontophoresis could be very helpful
because it will increase the absorption of medication and is a
method of driving KPV, or one other drug, deeper into the pores and skin, bypassing the
first metabolism within the intestine (Rawat S, 2008).
This peptide has been gaining popularity because of its potential in lowering inflammation, enhancing skin well being, and supporting general wellness, notably in people with persistent circumstances.
KPV has increasingly turn out to be well-liked amongst alternative
and integrative medication practitioners due to its broad therapeutic
results on inflammation and immune modulation.
Practitioners often highlight its efficacy in managing continual inflammatory situations,
enhancing wound restoration, and combating resistant
infections, although emphasizing the importance of additional clinical validation.
Larazotide is at present being studied for illnesses
of intestinal permeability and is the topic of a late-phase medical
trial for sufferers with celiac illness, whose intestinal barrier is compromised.
The mechanism of motion is due to the fact that Larazotide acts as an antagonist in opposition to zonulin, which is a
protein in the small gut that impacts gut permeability.
Zonulin creates areas in the “junctions” of the gut and by tightening up these spaces,
intestinal barrier perform can be restored.
Utilizing peptides may accelerate the skin’s pure therapeutic processes,
resulting in smoother and healthier-looking pores
and skin. As the skin regenerates, it turns into firmer,
more hydrated, and fewer susceptible to irritation or harm.
Most importantly, research proceed to highlight constructive findings around KPV peptide safety and side effects, making it a beautiful therapy to explore with skilled supervision. Chronic illnesses like Lyme can throw your
thyroid, adrenal, and even sex hormones into chaos. The KPV peptide is understood to affect these techniques, helping restore equilibrium the place it’s needed most.
Whereas this doesn’t work in a single day, the peptide’s regulatory properties could be a game-changer for long-term well being.
The benzyl alcohol has no toxicity at these concentrations, while it might possibly successfully suppress the growth of microorganisms.
Can the weight-reducing energy of Cagrilintide makes use of be
combined with the tissue-repairing properties of a compound like
GHK-Cu Copper Peptide, which we offer at Actual Peptides, to create a
holistic analysis protocol? We ensure researchers have access to a variety of high-purity peptides to
facilitate these complex comparative studies. One Other
vital analysis query addresses the synergy between Cagrilintide
and different compounds. Given that metabolic regulation is a multi-hormone course of, scientists
are exploring combination therapies. For occasion, research are carried out to
see how the appetite suppression results of Cagrilintide compare
or mix with the actions of GLP-1 analogues.
KPV can be one life-changing peptide when it comes to faster healing from injuries for individuals concerned in health,
sports activities, or bodybuilding. Learn via the tip to know every little thing associated to KPV, and I am pretty certain that it is feasible for you to to determine by the end whether to
use this peptide or not. These results are as a end result
of its suppression of inflammatory mediators and restoration of skin barrier perform.
Your probabilities of fulfilling these criteria depend in your
doctor’s willingness to have you strive what’s effectively an experimental drug.
To that end, there are respected clinics in the
Usa that prescribe KPV and different restricted peptides,
though they usually don’t deal in telemed or ship their remedies.
If you do decide to take Anavar on an empty stomach,
make sure to drink plenty of water to help stop any potential abdomen upset.
Anavar also can impact cholesterol levels, decreasing HDL (good) ldl cholesterol and growing
LDL (bad) cholesterol. This is more prone to happen in people who have already got hypertension or different cardiovascular
issues. When planning your Anavar cycle,
you will need to think about your goals and modify
your dosage and cycle length accordingly. If you
wish to bulk up, you could need the next dosage and longer cycle.
On the opposite hand, Anavar is an artificial steroid that can trigger significant hurt to your physique over time.
Throughout Anavar’s kick-in time, customers might
experience some instant results, such as elevated energy and endurance.
However, the complete effects of Anavar will not be noticeable till after a number
of weeks of use. Embracing this methodical approach
not only ensures a smoother integration of Anavar into your routine
but additionally lays the muse for a optimistic and transformative expertise.
In addition to muscle changes, this combination creates
an setting for efficient fat loss.
Conclusively, while Anavar is a strong tool for advancing bodybuilding targets, it doesn’t exchange the importance of good
coaching, balanced diet, and listening to
your physique. Sometimes, for male customers, a daily dosage falls in the vary of 30 to eighty mg.
Going above this suggested range might increase the chances of undesirable unwanted facet effects.
Importantly, taking a better dose doesn’t necessarily correlate to more vital features and may put additional stress on the user’s system.
While Oxandrolone, generally often identified as Anavar,
provides many advantages, it’s essential to grasp
it’s not with out drawbacks. One noteworthy downside is its potential to pressure
the liver. Anavar is an oral steroid and is metabolized via the liver.
Dianabol is a strong steroid that can be used for pre-workout functions.
Nevertheless, there are a selection of side effects that customers should be
aware of before taking the drug. Not solely will this result in larger and stronger muscle tissue, however it could also assist to
enhance your athletic efficiency. We’ll additionally cover a number of
the potential unwanted effects of this supplement and tips on how to keep away from them.
T3 is a thyroid hormone that has been proven to
be a robust fat-burning hormone. Regardless Of
the fact that Anavar is exogenous testosterone (as are all different steroids), it outperforms the competition when it
comes to fat burning. Anavar can also be an efficient fat burner because of its capability to extend T3 ranges within the physique.
Anavar use by women leads to a lower in pure testosterone
ranges. Although this will likely not seem like a major issue, women who have had a interval have reported feeling a lot
worse and having a decrease libido.
The aim of TRT is to restore testosterone levels to
the traditional physiological vary. Typical TRT dosages for men vary from 100mg to 200mg of testosterone per week,
divided into smaller doses administered either via injections,
gels, patches, or pellets. Anavar with TRT is an ideal combo because it could assist to extend muscle mass whereas also
lowering the side effects of TRT.
When utilizing this aggressive PCT, we sometimes see endogenous
testosterone manufacturing recover after 2 months. Selling steroids can outcome in up to 5 years in jail and a fantastic of $250,000.
He also recommends splitting up the doses of Anadrol throughout the day instead of taking
25 mg in one go. In some individuals, Anadrol could not produce the same fixed euphoria as Dianabol, for instance.
This is because Anadrol is a harsher steroid, so the unwanted effects
are more distinguished. Moreover, performing a sufficient warm-up will assist the muscular tissues
turn into more supple and reduce the risk of injury. DHT causes miniaturization of the hair follicles,
causing them to thin and even fall out.
Cardio generally gets a foul rap in the bodybuilding world, but it’s far more necessary than most people suppose.
Past just burning energy, it helps keep your coronary heart wholesome,
boosts endurance, and even accelerates restoration between exercises.
Done right, cardio won’t kill your gains—it’ll truly help them by preserving your physique lean, sturdy, and prepared
to push harder in the health club.
While many anabolic steroids cut back subcutaneous fats, they will also increase visceral fats.
As a result, steroid customers incessantly seem bloated or chubby (despite being
very lean). This is very seen in competitive bodybuilders, who regularly have a bulging steroid gut.
A perfect Anavar cycle will result in an 8-week increase in muscular firmness and definition. The majority of customers begin with a two-step dosage that allows the body to maintain the identical levels of the chemicals in query.
when to take anavar before or after workout
the levels of the hormone in the blood plasma are maintained, the steroid performs higher.
When Anavar is run in the proper dose distribution, its efficacy is increased.
A 2004 evaluation in Sports Activities Medicine documented estrogenic unwanted side effects of Dianabol 3.
Water retention and gynecomastia happen in 65-70% of users without
correct estrogen control. Another research printed in Hepatology demonstrated the hepatotoxic
results of 17-alpha alkylated steroids like Dianabol 2.
In younger animals, growth hormone deficiency may find yourself in bodily and cognitive
abnormalities that might be improved with growth hormone
alternative therapy. Maintaining sufficient development hormone levels promotes fats loss, muscle mass, muscle tone, and
weight loss. Decreased progress hormone ranges are correlated
with a rise in visceral fats discount and reductions in muscle
strength, endurance, and muscle loss. Thus, enhancing
growth hormone ranges and addressing elevated gh levels by way of
research can handle varied age-related declines.
Weight Problems and insulin resistance blunt each basal GH secretion and
secretagogue responses. People with higher visceral fats or impaired glucose tolerance sometimes see smaller will increase in GH/IGF-1 from the
same dose. Enhancing insulin sensitivity (dietary sample, weight
loss, physical activity) typically improves responsiveness more than growing dose.
Small proof-of-concept trials evaluated intravenous ipamorelin for postoperative ileus after bowel surgery.
Dosing schedules produced expected GH pulses and acceptable
short-term tolerability, but the important thing medical endpoint—speeding the return of
gut function—was not significantly better than placebo in the
major evaluation.
Up To Date Well Being Center and Men’s Modern Well Being Heart are both trusted well being facilities for men and women who are exhibiting signs of growth hormone (GH) insufficiency.
We ship superior treatment for girls combating low
hormones and males who’re combating low T and GH levels in Fort Myers and Naples.
Our suppliers try to make you are feeling protected and work
with you to create an effective therapy routine and supply lifestyle improvement ideas that can assist you reduce or get rid of the symptoms of development
hormone deficiency.
By stimulating the discharge of GH, it can accelerate
the body’s pure tissue repair processes. This may be particularly advantageous for individuals recovering from accidents, surgeries, or strenuous exercises, as it may facilitate
faster healing and scale back downtime. Sermorelin peptide remedy,
renowned for its distinct role in anti-aging and general well-being,
operates by stimulating the body’s pure production of growth hormone (GH).
Claims of dramatic fat loss, large muscle features, or superior sleep from
ipamorelin alone usually are not borne out by high-quality trials.
For children or adults with diagnosed GH deficiency, standard-of-care therapies—not secretagogues—govern therapy.
And for weight reduction, ghrelin agonism can enhance urge for food,
which may counter goals.
As at all times, particular person preferences, objectives, and medical guidance should dictate the selection between these peptides.
The right choice is dependent upon your health targets and tolerance for potential unwanted side effects.
CJC 1295 emerges as a useful asset for people striving
to harmonize their hormonal equilibrium and understand focused health and fitness
goals.
Since both of those are potent stimulators of muscle growth and growth hormone launch, stacking them collectively can even help in growing endurance,
particularly throughout workouts. Ipamorelin is a selective ghrelin receptor agonist—or
in less complicated terms, a peptide that mimics the hormone ghrelin to set off the release of growth hormone from the pituitary
gland. In Distinction To some earlier-generation GHRPs (like GHRP-6
or GHRP-2), Ipamorelin doesn’t jack up your cortisol or prolactin levels, which means you
may get the GH enhance without the hormonal rollercoaster.
Its shorter length of motion signifies that it more closely mimics the body’s natural pulsatile release of progress hormone.
When administered, what does sermorelin and ipamorelin do binds to GHRH receptors on the pituitary gland, stimulating the manufacturing and release of development hormone.
This increase in growth hormone can result in varied potential advantages, including improved physique composition, enhanced sleep quality, and
elevated power levels.
The utilization of subcutaneous injections is a widely accepted technique for administering peptides, offering environment
friendly absorption into the bloodstream. It is imperative to seek guidance
from a healthcare professional or an individual well-versed
in peptide therapy to establish the optimum administration regimen. On the opposite hand, CJC-1295, a progress hormone-releasing peptide,
stimulates the production of growth hormone and insulin-like progress factor 1.
Research has proven that CJC-1295, a synthetic peptide, can stimulate
the production of progress hormone within the
physique, resulting in increased muscle growth and enhanced restoration after physical activity.
GH and IGF-1 stimulate pores and skin cell regeneration and
collagen production, probably enhancing firmness,
tone, and hydration—especially when mixed with life-style changes and adequate protein intake.
“Exogenous GHRH administration enhances slow-wave sleep and GH release, bettering subjective sleep quality”(Born et
al., Neuroscience Letters). Mechanistically, Ipamorelin binds to the GHS-R1a receptor, mimicking ghrelin to enhance
GH secretion. Nonetheless, not like ghrelin or older peptides, it
avoids undesirable unwanted facet effects — making it one of the cleanest GH secretagogues obtainable.
Our chosen compounding pharmacy will the injection medicine and injection provides
to your home.
Sermorelin is often the go-to peptide for anti-aging
as a result of its gradual and sustainable influence on skin elasticity, energy ranges, and total
vitality. Peptides like Sermorelin and Ipamorelin activate
the hypothalamus and pituitary gland to release HGH, aiding in development hormone deficiencies and offering anti-aging benefits.
Long-term use of both peptide must be monitored intently by a healthcare supplier.
If sustainability is a concern, Sermorelin might offer
more holistic benefits.
I would like to understand how a lot bacteriostatic water ought to
be added to a 10mg vial of the peptide combine to
realize a 300mcg dose. I will dedicate my time to provide you
with excellent service and help. When trying to safe a research-grade provide of Sermorelin or Ipamorelin, don’t overlook to acquire the materials required for proper reconstitution, storage, and
administration. To help researchers, our team made a collection of check purchases from
various vendors and rated them based on price, transport times, and customer support.
In the subsequent part, we’ll focus on what ipamorelin is and the kind of
benefits it offers when administered to test subjects.
A customized care plan encompasses not solely the dosage of the mix but also concerns such as the frequency of
administration and any potential interactions with other medications.
Individuals who have built-in this mix into their well being regimen have reported heightened sexual satisfaction and endurance.
By stimulating the body’s innate production of growth hormone, Sermorelin Ipamorelin can contribute to a extra gratifying and fulfilling
sexual expertise. Intelligent peptide stacks produce effects higher than the sum of their individual advantages.
They address the body’s interconnected methods (ie hormones have an effect on sleep,
sleep impacts metabolism, and metabolism impacts inflammation).
Additionally, Ipamorelin stands out for its selectivity in stimulating development hormone
release with out affecting cortisol or prolactin levels significantly.
Ipamorelin and Sermorelin exhibit distinct differences in their mechanisms of motion,
particularly regarding development hormone secretion patterns, body
weight effects, and urge for food regulation.
At the receptor level, ghrelin agonists need the receptor’s distinctive binding pocket that acknowledges
ghrelin’s acyl modification. Advances in structural biology over the final few years have clarified how the receptor acknowledges this acylated hormone and how small variations in ligands can change signaling.
In abstract, each sermorelin and ipamorelin present
clear potential for the treatment of hypogonadism in men and the lack of available data opens
alternatives for future investigation. In Contrast with ipamorelin, there might be more knowledge about sermorelin’s impact
on long-term well being and this could make it appealing to
safety-conscious researchers.
On the other hand, Sermorelin directly influences the pituitary gland to launch growth hormone, which aids in combating the consequences of aging by enhancing muscle mass and bone density.
Whereas both peptides offer rejuvenating benefits, their distinct mechanisms provide a tailor-made strategy
to combating the indicators of growing older for people
looking for particular outcomes. Sermorelin triggers growth hormone release,
and the liver converts it into IGF-1. Over weeks and months, IGF-1 supports fat
loss, elevated muscle tone, and enhanced recovery.
Studies have shown that Ipamorelin may help in lowering inflammation, enhancing the quality of sleep,
and even supporting higher pores and skin elasticity. This peptide’s effectiveness is often seen in rising muscle mass,
improving bone density, and aiding in damage recovery. In contrast, Ipamorelin specifically targets growth hormone receptors, stimulating progress hormone
secretion with out exerting significant effects on the levels of different hormones.
After this assessment, healthcare providers can meticulously determine the initial dosages of Sermorelin Acetate and Ipamorelin. As the therapy progresses, adjustments to the dosages may become essential to optimize the therapy’s efficacy and decrease potential unwanted effects.
The pure elevation of progress hormone manufacturing via Sermorelin Acetate
can lead to decreased body fats and enhanced skin elasticity, thereby contributing to a more youthful appearance.
This method makes it a preferred possibility for
long-term health optimization. Ipamorelin offers quick, direct
stimulation of growth hormone with minimal impression on other hormones like cortisol.
CJC 1295 works extra gradually by stimulating your pure growth hormone production over a longer period.
Some people select to mix both for extra sustained and enhanced outcomes, especially in anti-aging and muscle-building protocols.
At PeptidesPower.com, we’re devoted to providing top-quality peptides, hormone therapies, and wellness dietary
supplements to assist your well being, health, and recovery goals.
Yes, ipamorelin is commonly used as a half of a weight loss program as a result of it helps
enhance progress hormone ranges, which can boost metabolism,
scale back body fat, and support lean muscle retention. While it’s not a weight reduction drug
on its own, it’s generally included in medically supervised
protocols for fat loss and body composition enhancements.
Sermorelin and Ipamorelin act as peptides to set off
development hormone launch but operate differently.
It makes the pituitary gland launch progress hormone by copying pure GHRH.
A key difference exists with Ipamorelin – a selective ghrelin receptor agonist that instantly
causes growth hormone release when it binds
to ghrelin receptors. But Ipamorelin typically
proves more selective with actually minimal side effects,
especially for appetite changes.
“Peptides are a pure extension of the work we already do in hormone and wellness drugs,” stated Wayne Wilson, Founder and CEO of SynergenX.
“By expanding our peptide therapies we’re giving patients cutting-edge assets to recover, restore, and thrive so they can achieve s higher high quality of life.” This distinction in their mechanisms of motion can affect their efficiency and effectiveness in promoting progress hormone secretion. Its role in anti-aging processes has additionally gained consideration,
as it could help the upkeep of muscle and tissue well
being whereas providing a youthful vitality to the physique.
It is crucial to note that these reactions are usually mild and transient, resolving on their
very own as the physique adjusts to the treatment.
In uncommon circumstances, extra severe side effects such as allergic reactions or changes in blood sugar ranges might happen,
necessitating immediate medical attention. By adhering to those precautionary protocols, healthcare professionals can preemptively address any challenges
that may come up and optimize the therapeutic outcomes of Sermorelin Acetate and Ipamorelin remedy.
References:
https://git.k8sutv.it.ntnu.no/
buy legal anabolic steroids
References:
https://rearch.engineer
does rich piana take steroids
References:
videyme.online
which of the following has been found to be a side effect
of anabolic steroid use?
References:
corerecruitingroup.com
Not solely do we see users’ muscle fibers increase in dimension, but
they also restore faster than before because of enhanced restoration levels.
This can allow bodybuilders to coach for longer durations of
time without fatiguing or overtraining from strenuous workouts.
In terms of weight acquire, it’s widespread for users
to achieve 20 kilos within the first 30 days on Dianabol
(3). Most of this might be within the type of muscle mass (plus
some water retention). Pimples tends to seem alongside the chest, face,
neck, again, and arms in response to excessive doses of steroids, in accordance with the DermNet.
The Eastern-bloc weightlifters and monitor athletes subsequently dominated the athletic stage for decades.
Steroids are a general class of brokers that all have the steroid ring in widespread.
The steroid ring consists of three 6-carbon rings and one
5-carbon ring joined, of which cholesterol is essentially the most fundamental kind and, certainly,
the precursor. Though the time period steroid consists of all agents derived from this ringed structure,
this dialogue contains solely testosterone and the anabolic-androgenic steroids (AASs).
Some teens tackle intense training, have an excessive level of physical development
already, and have come to a genetic wall. In these cases, guys may start on gear
at 20, however you’d need an excellent
cause to do it. The half-life of each ester is one of the main differences between them.
The time course and components affecting HPGA recovery after cessation of use are poorly characterised.
Blood exams can be performed to verify the person’s present degree of testosterone and determine whether it’s greater than regular.
Blood levels of different reproductive hormones (such as follicle stimulating hormone [FSH], luteinizing hormone [LH]) can be measured.
If the testosterone could be very excessive however
the FSH and LH ranges are low, this provides evidence
that the individual is using anabolic steroids. Anabolic steroids act
at androgen receptors to affect mobile functioning and gene expression. In 1953, a testosterone-derived steroid
generally identified as norethandrolone (17α-ethyl-19-nortestosterone) was synthesized at G.
Each time you eat food, the liver has to digest
it; thus, when taking hepatotoxic steroids and
eating giant quantities of meals, the liver is changing into increasingly taxed.
The body’s method of dealing with that is
to suppress the person’s appetite (as a self-defense mechanism), lowering meals consumption. Due to Dianabol’s
aromatization effects and being highly estrogenic, it’s a compound that causes vital quantities of water retention. This can go away users looking puffy, bloated, and smooth-looking; therefore, why
it’s sometimes used within the off-season.
The researchers found levels returned to normal about four months after participants stopped taking them.
The potential for vital hepatotoxicity from Winstrol necessitates comparatively temporary cycles to prevent excessive liver injury.
Winstrol, when stacked with further oral steroids, increases the
risk of jaundice or liver cholestasis (impaired bile flow).
Trenbolone is thought to considerably cut back fats mass while facilitating muscle growth.
Some bodybuilders additionally make use of trenbolone as a slicing steroid to speed up fats
loss while sustaining muscle on fewer energy.
Anavar side effect prevention tips and testosterone are widely considered the least harmful anabolic steroids concerning cholesterol.
In our expertise, the cardiovascular strain of Anavar is marginally greater than that of testosterone.
We have found that bodybuilders on Dianabol can experience an increase in vascularity.
This is when the veins turn out to be more visible, often seen spiraling by
way of a person’s muscle tissue, resembling a human roadmap.
As a results of this additional blood move, pumps can turn into
noticeably bigger during exercises as a outcome
of increased N.O.
This has significant benefits but additionally offers you some sense of invincibility, however again, most customers are still finest suggested to stick with normal rep ranges for injury avoidance.
Some steroids, like Deca, are distinctive at serving to heal injury and constructing cartilage,
however no compound will make you indestructible or resistant to new injuries.
Steroid stacks combine two or extra compounds so you possibly can combine their benefits
and achieve larger outcomes than utilizing only one compound alone.
Newbie stacks can be simple, while advanced customers can simply mix three or more
compounds in a cycle. This is a 10-week cycle; however
(very important) – Anadrol should only be used for the first three weeks!
Dianabol is a beginner-friendly oral steroid, providing Quick Techniques to Make Veins Pop Out Quickly results,
but it ought to be used with caution because of its potential liver
toxicity. Beginners also have to be aware the doses that are appropriate for them won’t be as high as these utilized by more experienced steroid customers.
The beneficial CrazyBulk Winstrol dosage for newbies sometimes ranges from 20 to 50 mg
per day over 6 to 8-week cycles. This makes extra circulating testosterone
available to support muscle development and improve efficiency.
In addition to doing these things, Testosterone
Enanthate additionally supports the production of purple blood cells.
Good bodybuilding isn’t nearly lifting heavier or consuming cleaner—it’s about understanding the inner systems that power each motion. Monitoring electrolyte levels, adjusting consumption based
mostly on training intensity, and using targeted
supplementation may help athletes keep ahead of fatigue,
cramps, and efficiency plateaus. When you sweat
via grueling classes, your physique loses not simply water however vital electrolytes.
Without correct replenishment, the implications can vary from gentle fatigue and muscle cramps
to severe dehydration and impaired efficiency. Sodium and potassium, in particular, play a dynamic function in maintaining cellular hydration and ensuring muscles contract and chill
out effectively.
To velocity up recovery and get again to peak performance, many are turning to healing peptides like BPC-157 and TB-500.
These compounds are gaining attention for their potential to accelerate tissue repair, reduce inflammation, and help total healing.
This article takes a closer take a glance at how each peptide works, compares their advantages, and
explores which might be higher suited for harm restoration in high-performance athletes.
Your health care supplier will let you know should you ought to stop breastfeeding or cease oxandrolone.
Tell your health care supplier in case you are pregnant or plan to turn into pregnant.
If you turn out to be pregnant, stop taking oxandrolone immediately and make contact with your health care provider.
Before taking oxandrolone, tell your well being care supplier
about any prescription or over-the-counter (OTC) medicines,
vitamins/minerals, natural products, and different dietary supplements you’re using.
Tell your health care provider about all of your health conditions and any prescription or over-the-counter (OTC) medicines, vitamins/minerals, herbal products,
and different dietary supplements you are using.
Because the “come down” on Anadrol is extreme,
we typically see steroid customers opt for a milder steroid corresponding to Deca Durabolin after coming off to help this transition. Such a protocol
may also help customers retain more strength and muscle gains skilled from an Anadrol cycle.
Due to Anadrol’s drastic impact on HDL cholesterol levels, water retention,
and pink blood cell rely, it is a steroid that has a unfavorable effect on the heart.
Beyond pharmacological interventions, lifestyle factors also play an important position in recovery.
Sufficient sleep, proper vitamin, and stress administration are important for supporting hormonal stability
and overall well-being.
One Other study found psychological effects after 14 weeks of 500 mg administration of testosterone cypionate for
week [18]. Furthermore, a current examine discovered that in a inhabitants of AASs users the weekly dose assumption ranged 75–1550 mg/week
[20]. Speak to your well being care supplier about tips on how to keep healthy blood sugar
ranges.
Alcohol must also be prevented, and stacking hepatotoxic steroids together, such
as Dianabol and Anadrol, just isn’t beneficial.
Beneath is a table evaluating the detection time of oral vs.
injectable steroids. In this text, we analyze the professionals and
cons of oral vs. injectable steroids so you understand what to
anticipate and which method of administration is perfect for
you.
Your steroid cycle construction might need to incorporate either a kickstarting compound or the method of frontloading.
This might be important when you’re utilizing a quantity of gradual appearing (long ester) steroids which have
long half-lives. Without a kickstart or frontloading,
you will be ready weeks to see outcomes with steroids like Deca-Durabolin and Equipoise, which are well known for his or her lengthy
half-lives. So, you possibly can see the significance
of familiarity with each compound’s half-life, even if you’re
going with just a single compound cycle. By understanding esters,
you could be in the best place to create efficient
steroid cycles with compounds that complement each other
based mostly on their completely different half-lives and
onset of results. The downside to this cycle is that it’s notably cardiotoxic, with blood stress
rising considerably. Users can incorporate
common cardiovascular exercise into their schedule to
reduce back cardiac pressure.
Anadrol can be one of the highly effective compounds for enhancing power, making it very popular among strongmen and
powerlifters, in our experience. Safer options like the most effective oral steroid with
least unwanted facet effects or most secure steroids for over 50 should always be prioritized.
We considered security ratings primarily based on effects
on ldl cholesterol, hair loss, and total unwanted facet effects.
This reduces the chance of estrogen-related unwanted side effects,
making them safer. Anavar is usually cited because the
most secure oral steroid due to its light profile. Turinabol is commonly
used by skilled athletes who compete in tested federations.
With your metabolism working more efficiently, your body can’t
help however burn body fat, particularly when you’re on a calorie deficit food plan while cutting.
Though far from a muscle-building compound, Clen will help
forestall muscle wastage whereas slicing, because of its minor anabolic properties
that mildly enhance protein synthesis. Clen boosts
the metabolic price, which at its core is caused by
increased physique temperature (this contributes to
some attainable side effects). Some users discover the metabolic effects wane
with continued use, so a two-week on and two-week off routine is commonly very efficient.
This quick-acting oral steroid additionally leaves the body shortly,
so you have to take it daily. It ought to be used for not than 6 weeks, but
even four weeks will give excellent results at 50mg every day.
When these shoot up, it is evidence of liver stress; thus,
regular checkups with a doctor ought to be taken to closely monitor these scores.
Any excess fluid gained from Anadrol shall be flushed out when a cycle finishes and estrogen ranges return to normal.
Anadrol is also some of the highly effective compounds for enhancing strength,
making it extremely popular amongst strongmen and powerlifters, in our
expertise. In sure instances of addiction, patients have taken medicines to assist treat symptoms of withdrawal.
For instance, well being care suppliers have prescribed
antidepressants to treat melancholy and pain medicines for complications and muscle
and joint ache.
One Other steroid that is typically taken orally, methylprednisolone is used to treat
more critical situations similar to blood disorders, lung ailments,
and a few forms of cancer. Like prednisone, the primary operate of this steroid is to decelerate the immune system’s
response to those various circumstances and cut back their subsequent signs.
Thanks to high-profile circumstances of illicit misuse in sports,
steroids have turn out to be synonymous with dishonest.
However, steroids are also prescription drugs that can be utilized to deal
with a selection of frequent situations. The
primary targets of medication-assisted therapy are to
help alleviate withdrawal signs, prevent relapse, and restore hormonal stability.
Turinabol provides its performance-enhancing effects by growing red blood cell count, which supplies the
muscular tissues more oxygen and vitamins, further boosting their endurance and
power. Rising Impact whey protein safety synthesis and nitrogen retention will
increase anabolic activity, so lean muscle is retained.
For cutting purposes, a better dosage holds little profit but a better threat of unwanted effects.
Subsequently, as little as 200mg weekly, as much as 400mg weekly is really helpful.
An 8-week cutting cycle with Equipoise is beneficial, together with in case you are doing a longer cycle with other
compounds; use EQ for the primary eight weeks. Equipoise excels at cutting and is great
at serving to retain lean muscle and provide a common improvement in physique
conditioning. Energy, muscle endurance, and recovery
enhancements are areas in which Equipoise supplies exceptional benefits.
In the Usa, an AAS is a schedule III controlled substance obtainable solely
by prescription. The use of those medication is only authorized when a medical professional prescribes them.
Some AASs solely have medicinal makes use of, similar to testosterone undecanoate
(Nebido). Oxymetholone (Anadrol) is an instance of a
steroid with both medicinal and performance
makes use of.
As bodybuilders who use steroids, certainly one of our
highest priorities is to maintain a excessive and fixed blood
plasma degree of all steroids being utilized in a cycle.
When you’re using one of many sluggish appearing (long ester) steroids,
it ends in a slower build-up of the steroid over a longer interval and, due to this fact,
slower results. So, you presumably can see the importance
of familiarity with every compound’s half-life, even if you’re going
with only a single compound cycle.
Some of those steroids can exit the physique within the urine without having been metabolized, producing a strong optimistic end result for a protracted interval of a quantity of months.
Your dosage and the way lengthy you use a steroid will
decide your threat of voice changes and, specifically, just how deep your voice could get.
It starts slowly, with a noticeable but typically intermittent crackling or hoarseness of the voice,
which you may mistake for an sickness. However different individuals will soon begin to discover your vocal
change if it progresses with continued steroid use.
The most common muscle injection websites are those of the larger, stronger muscles
just like the thigh and buttock. Over time, you might develop a
preference for which muscle tissue you inject in relying on which compounds you’re using and the pain stage.
The proof around whether or not anabolic steroids can considerably enhance athletic efficiency is limited eight.
But typically speaking, there has been some research which
has shown that people who use anabolic steroids will experience a rise in muscle strength 9.
There is a dosage-dependent effect of anabolic
steroids on muscle mass and power 65, sixty six.
The dose-response curve for anabolic steroids has not been clearly outlined, however male athletes and body builders
often use mega dosages 28. They additionally typically use a selection of anabolic steroids concurrently
(“stacking”) or sequentially (“cyclically”) because of a belief that these
regimens are safer 28. With the exception of some elite feminine
athletes and body builders, women seldom use supraphysiologic dosages of
anabolic steroid.
It’s technically not a steroid per se, however because it has
similar effects, it is used as such. With the rise of e-commerce, online
steroid suppliers have become more and more well-liked in Australia.
Nonetheless, not all on-line suppliers are created equal,
and it’s important to supply from reputable and legal sources.
Steroid use may usually contain polypharmacy –
where an individual mixes a number of substances to enhance results,
manage unwanted effects, or obtain particular aesthetic or efficiency objectives.
Yes, SARMs can present up on drug exams, particularly those
designed for anti-doping purposes in sports activities.
TestoPrime claims to burn fat, improve muscle constructing and enhance mental and bodily energy.
All this with minimal unwanted facet effects and certainly a lot much less danger than anabolic steroids.
At the top of the record of the best legal steroids in Australia is Clenbutrol.
Ostabulk is brutal Force`s legal different to get the muscle
features and physique fat loss that Ostarine offers.
It has a strong list of ingredients, however I`ve received
combined suggestions from my prospects about its effectiveness.
It is unlawful to import, promote, supply or promote peptide hormones
without a valid prescription from a licensed
medical practitioner.
It is also necessary to assume about safer and authorized options, corresponding to
authorized steroids, earlier than making any decisions.
These products are made from natural ingredients and should provide similar results to traditional
anabolic steroids. When buying steroids in Melbourne,
it’s essential to make certain that the merchandise are legally obtainable for purchase.
If you’re looking to purchase steroids in Melbourne,
it’s necessary to grasp the legal tips surrounding their
acquisition.
When individuals use multiple steroids simultaneously, a practice known as “stacking,” it can increase the probability of experiencing adverse effects.
The interplay between totally different substances within the body is complex and never absolutely understood, making it essential for users
to be aware of potential risks. In Australia, the authorized
status of steroids is clear – they are solely authorized if prescribed by
a doctor for medical causes. Possession, use, sale, or
distribution of steroids without a prescription is towards the law and can lead to severe penalties, together
with imprisonment. The penalties for supplying steroids vary
throughout totally different states and territories, with some classifying them in the same drug class as heroin or ice.
Where a possession offence includes lower than a traffickable quantity,
an $8,800 fine (50 penalty units) may as an alternative be applicable.
Army refers to the armed forces and their role in defending national security
and interests. This class includes metrics similar to
navy spending, troop energy, equipment and technology, and readiness
for combat. This category consists of metrics such as historical landmarks, museums, and archaeological websites.
These medication are commonly used to promote muscle progress, improve power, and cut back
recovery time after injuries. Anabolic steroids differ from corticosteroids, which are
used to deal with circumstances like arthritis or asthma.
Going Through costs for the penalty for possession of steroids in Australia is a severe
matter that may influence your future significantly.
If you may be facing charges associated to steroids in Queensland, whether
for possession, provide, or importation, the experience
of Visitor Lawyers can be invaluable. Our experienced team
is ready to present professional authorized advice and sturdy illustration to make sure
the very best end result in your case. To
guarantee security, anabolic steroids should solely be used under the supervision of a well being care provider.
Steps could be taken to reduce the chance of unwanted effects, such as lowering the
dosage, limiting the period of use, and using clear needles
to stop infections.
In South Australia, anabolic steroids are categorized as a controlled substance under the Managed Substances Act 1984.
The possession, use, and supply of anabolic steroids without a prescription are illegal.
It is important to note that steroids are legal for medical purposes
when prescribed by a licensed medical practitioner.
Sometimes, steroids are prescribed to treat circumstances such as delayed puberty,
muscle loss as a end result of most cancers or HIV, and hormonal imbalances.
To acquire a prescription, patients should endure a radical medical examination to find
out if steroids are necessary for their remedy plan. Having spent years within the fitness
industry, I’ve witnessed firsthand the allure of
anabolic steroids and the influence they will have on people.
While some might argue that steroids present a shortcut to success, the truth is often rather more
advanced. Users typically face challenges in verifying the authenticity and security of the products they buy.
Counterfeit steroids can include dangerous substances
or incorrect dosages, posing significant well being dangers.
Moreover, engaging in the underground market can lead to legal repercussions if caught.
With us you ought to purchase fat burners from different producers,
together with the most well-liked merchandise from athletes around the
globe. There is a pharma for different purposes, for example, to extend strength, endurance and sexual exercise.
Competent selection of medication, above all, a big increase in the outcomes of bodily exertion, the motivation to
continue training and glorious mood. The athlete turns into a lot sturdier, can do
more approaches and reduce the time between them, after considerable bodily
exertion he wants much less time to get well. Anabolic steroids have been used by athletes in many professional
sports activities, including observe and field, weightlifting, bodybuilding, shot
put, cycling, baseball, wrestling, mixed martial arts, boxing, and soccer.
Such use is prohibited by many of the skilled and novice associations
that arrange these sports. Crazybulk is a reputable company that sells authorized steroids
which might be protected and effective.
References:
Simple Starter Regimen
legal steroids that really work
References:
support.roombird.ru
are steroids legal in brazil
References:
https://aryba.kg/user/coffeeseason9/
garcinia pills free trial
References:
u.to
how much hgh
References:
4 iu to mg hgh (generation-n.at)
anabolic steroid users
References:
https://www.youtube.com/redirect?q=https://pedselite.com/hgf-max-review-what-to-expect-from-this-hgh-supplement/29495/
hgh dosage bodybuilding
References:
hgh 3 months results (https://www.askocloud.com/)
how long to take hgh for bodybuilding
References:
Is hgh or Testosterone better (oiaedu.Com)
hgh dosage iu bodybuilding
References:
dosage of hgh for bodybuilding (https://md.ctdo.de)
hgh hormon abnehmen
References:
hgh fat loss dosage – xypid.win –
hgh dosage iu
References:
Genfx Hgh (Lovewiki.Faith)
hgh nebenwirkungen team andro
References:
hgh dosage for injury recovery (http://cqr3d.ru/user/daisyshark09/)
hgh dosage for height increase
References:
hgh Dosage calculator (https://odvinsk.ru/)
side effects of hgh injections
References:
Hgh steigern, https://Avtovoprosi.Ru,
does skipping increase hgh
References:
difference between testosterone and hgh [pad.stuve.uni-ulm.de]
hgh hormone injection side effects
References:
hgh iu Per day [e1Adphegqz7e.рф]
hgh injektion
References:
before after hgh (jobgetr.com)
hgh day
References:
hgh Zum abnehmen, https://doodleordie.com,
Đến với J88, bạn sẽ được trải nghiệm dịch vụ cá cược chuyên nghiệp cùng hàng ngàn sự kiện khuyến mãi độc quyền.
hgh dosage for height increase
References:
Hgh vs anabolic steroids, bookmarkzones.trade,
street name for anabolic steroids
References:
enregistre-le.top
steroid to build muscle fast
References:
https://myspace.com/railmuseum24
hgh for beginners
References:
4iu hgh reddit (middleton-garrett-2.blogbright.net)
dosage of hgh for bodybuilding
References:
hgh bad for you (http://Www.generation-n.at)
anavar vs hgh
References:
hgh x2 somatropinne (http://Www.divephotoguide.com)
guia hgh
References:
hgh bijwerkingen (https://ondashboard.win/)
wat betekend hgh
References:
hgh nebenwirkungen team andro (https://vacuum24.ru/user/profile/427810)
苹果签名,苹果超级签平台,ios超级签平台ios超级签苹果企业签,苹果超级签,稳定超级签名
hgh results
References:
2 iu hgh per day results bodybuilding (https://muir-douglas-3.mdwrite.net/winstrol-depot-en-espana-compra-y-venta-online)
hgh frauen bodybuilding
References:
Jintropin hgh (https://Wasl.tech/forums/users/eyedigger29/)
hgh jintropin
References:
guía hgh (https://urlscan.io/result/019a71d1-51df-746e-8f29-29f09c74358c/)
Tham gia cộng đồng game thủ tại Go88 để trải nghiệm các trò chơi bài, poker phổ biến nhất hiện nay.
Khám phá thế giới giải trí trực tuyến đỉnh cao tại MM88, nơi mang đến những trải nghiệm cá cược thể thao và casino sống động.
iwin – nền tảng game bài đổi thưởng uy tín, nơi bạn có thể thử vận may và tận hưởng nhiều tựa game hấp
Với giao diện mượt mà và ưu đãi hấp dẫn, MM88 là lựa chọn lý tưởng cho các tín đồ giải trí trực tuyến.
Khám phá thế giới giải trí trực tuyến đỉnh cao tại MM88, nơi mang đến những trải nghiệm cá cược thể thao và casino sống động.
g casino bolton
References:
http://set.ua/bitrix/rk.php?goto=https://www.adscron.com/user/profile/2404
mahjong connect timeless
References:
http://polishcrazyclan.ugu.pl/member.php?action=profile&uid=385955
roulette system
References:
http://dle1.xn--31-6kc3bfr2e.xn--p1ai/user/bitineimyr
couple spa singapore
References:
https://deitglobal.com/leoraholyman1
south point casino las vegas
References:
https://skype.acenteyonetim.com/read-blog/48640_online-casino-freispiele-ohne-einzahlung-fur-dezember.html
casino el camino
References:
https://gitea.quiztimes.nl/adastocks32344
g casino reading
References:
http://101.35.201.220:3333/gayd8012395011
couple spa singapore
References:
https://social.updum.com/read-blog/32355_seriose-online-casinos-2025-liste-mit-seriosen-anbietern.html
hard rock casino hollywood
References:
https://gitea.noname-studios.es/darciovz901511
online casino biz
References:
https://git.yangzhiqiang.tech/madonnalayden
casino 770
References:
https://git.tablet.sh/alisiaprovost7
hollywood casino pa
References:
https://gitea.cncfstack.com/ahydorine19423
casino889 net
References:
https://amcompany.ir/read-blog/6558_vulkan-vegas-casino-bewertung-2025-test-amp-erfahrungen.html
south dakota casinos
References:
https://git.gonstack.com/candramccue654/candra2021/-/issues/1
du mobile
References:
http://94.224.160.69:7990/sterlingwinchc
craps for dummies
References:
http://osztromok.com:3164/craigmclamb359
le richelieu in the french quarter
References:
https://99link.me/LktTe
silversands casino
References:
https://wedeohire.com/employer/casino-mottoparty-kleidung-dekoration-und-spielideen/
sugar creek casino
References:
http://www.xn--3e0bl91azmcnwkspav10e.com/bbs/board.php?bo_table=free&wr_id=16218
Sie bieten einen ausgezeichneten Kundendienst, ein breites Angebot an Spielen von renommierten Herstellern und schnelle Auszahlungen. Das Zahlungsangebot ist oft vorzüglich und bietet lokale Optionen wie Paysafecard, Sofort und Giropay. Die Boni erfordern eine Mindesteinzahlung von 20€ und müssen innerhalb von 7 Tagen 35 Mal umgesetzt werden. Als Willkommensbonus kannst du zwischen 7 verschiedenen Optionen wählen, die wirklich alle Präferenzen und Spielstile abdecken.
Beachten Sie, dass es in der Auswahl von Live-Spielen in NVcasino online interessante Automaten mit bedingt «erotischem» Inhalt gibt. Ein interessantes Merkmal von NV casino online ist der Zugriff auf Testversionen von Spielen auch im Live-Bereich. Beachten Sie, dass die Vielfalt der Angebote im NV casino online an den Automaten nicht aufhört. Oben haben wir darüber gesprochen, dass NV casino online Automaten und Live-Spiele von mehr als fünfzig Anbietern von Spielsoftware enthält. Egal wann, wo und auf welchem Gerät Sie spielen möchten – das NV Casino ist auf Ihrem Handy und Tablet verfügbar. Die Mission von NV Casino beschränkt sich nicht nur darauf, Ihnen eine vertrauenswürdige und zuverlässige Spielplattform auf jedem Gerät zu bieten. Wie einfach, schnell und bequem ist es, in einem Online-Casino zu spielen?
References:
https://online-spielhallen.de/online-casinos-osterreich-kompletter-leitfaden-2025/
Die Dama N.V.-Casinos bieten zahlreiche Optionen, sodass Sie schnell und sicher Ein- und Auszahlungen vornehmen können. Einfache und sichere Zahlungsmethoden sind ein Muss für Online-Glücksspiele. Betsoft bietet auch Live-Dealer-Spiele an, die den Nervenkitzel eines echten Casinos direkt auf die Bildschirme der Spieler bringen und ein interaktives und fesselndes Erlebnis garantieren. Betsoft zeichnet sich durch seine außergewöhnlichen 3D-Slot-Spiele aus, die eine atemberaubende Grafik und ein fesselndes Gameplay bieten. Dama N.V. Casinos arbeiten mit den besten Softwareanbietern der Branche zusammen, um Ihnen ein erstklassiges Spielerlebnis zu bieten. Dama N.V. Casinos bieten ein reichhaltiges und vielfältiges Spielerlebnis, das auf Spieler aller Vorlieben zugeschnitten ist.
Dama N.V. Casinos bieten eine breite Auswahl an Tischspielen, die besonders für Spieler attraktiv sind, die gerne strategie- und geschicklichkeitsbasierte Spiele spielen. Zusätzlich zu den traditionellen Sportwetten bietet NVcasinos auch Wetten auf Cyber-Sportarten an. Solche Angebote wechseln aber ständig – wenn du also irgendwo einen nv casino Bonus Code ergatterst, check lieber auf der offiziellen Promotions-Seite, ob er noch gilt. Unser Willkommensbonus beträgt bis zu 2.000 € + 225 Freispiele. NV Casino bietet eine beeindruckende Auswahl an Casinospielen, die sowohl klassische Favoriten als auch moderne Highlights umfasst.
References:
https://ahiknuro.s3.amazonaws.com/casino%20b%C3%BCnde.html
Die besten Online Casinos bieten immer eigene Limits wie Einzahlungslimits und zusätzliche Systeme zur Unterstützung von verantwortungsvollen Spielen an. Wir erklären das Konzept des verantwortungsvollen Spielens und bieten Strategien und Hilfsmittel an, um deine Spielgewohnheiten effektiv zu kontrollieren. Anbieter mit Lizenz in Deutschland bieten dir diese Optionen direkt im Spielerschutzbereich an. Dabei lohnt sich der Blick auf die gesamte Spielauswahl. Die Spielbank ist bekannt für ihr elegantes Ambiente, den erstklassigen Service und die regelmäßig stattfindenden Pokerturniere, die Spieler aus aller Welt anziehen. Ein seriöses Online Casino besitzt eine gültige Glücksspiellizenz einer anerkannten Behörde. Mobile Casinos bieten eine nahtlose Spielerfahrung, egal von welchem Gerät.
Mehr Informationen zur Vertrauenswürdigkeit eines Online Casinos, zu diversen Zahlungsmethoden, Casinospielen und Registrierungsabläufen findest du hier bei uns, bei Casinoandy. Deshalb hoffen wir, dass wir von Casinoandy dir die Qual der Wahl etwas erleichtern können, und dass auch du anhand unserer Liste dein Lieblingscasino finden wirst. So wie sich das Wissen der Menschheit immer weiter entfaltet, entwickeln sich auch Spieler von Glücksspielen immer weiter. In beiden Fällen sind fast immer alle Spiele verfügbar und auch was den Kundendienst und die Transaktionen betrifft, verläuft alles mühelos über dein Mobilgerät, sodass du jederzeit und überall spielen kannst. Deshalb bieten nicht nur die neuesten, sondern auch bereits eingebürgerte Online Casinos eine mobile Version an.
References:
https://esijjohu.s3.amazonaws.com/jackpot%20frenzy%20casino.html
References:
Anavar before and after pics female
References:
http://humanlove.stream//index.php?title=pencilwish85
buying steroids online illegal
References:
https://menwiki.men/wiki/Clenbuterol_Achat_en_Ligne_Acheter_Clenbuterol_Sopharma_100_mg_0_02_mg
References:
Anavar cycle before after
References:
https://hedgedoc.info.uqam.ca/s/bLLMMG7I0
steroid injection for muscle growth
References:
https://notes.io/eugbB
%random_anchor_text%
References:
https://u.to/XWJyIg
david laid steroids
References:
https://firsturl.de/L6Ng3KI
References:
Casino new brunswick
References:
https://egamersbox.com/cool/index.php?page=user&action=pub_profile&id=258200
References:
Slot madness no deposit bonus codes
References:
https://pads.jeito.nl/s/Rc2J4uPZ4h
References:
Days inn clifton hill casino
References:
https://lovebookmark.win/story.php?title=candy-casino-built-around-flexible-payments-not-big-cashouts
anabolic supplements gnc
References:
https://mensvault.men/story.php?title=androtiv-gel-a-la-testosterone-40-sachets-unidoses
closest super supplements
References:
https://coolpot.stream/story.php?title=viagra-kaufen-ohne-rezept-legal-alles-was-sie-wissen-muessen
anabolic steroids can be ingested in which ways
References:
https://pailpoland7.bravejournal.net/se-descubre-una-relacion-probada-entre-el-fenogreco-y-la-testosterona
dianabol pills side effects
References:
https://menwiki.men/wiki/China_Human_Growth_Hormone_Powder_Suppliers_Manufacturers_Factory_Wholesale_Price
References:
Lucky eagle casino
References:
https://wifidb.science/wiki/Access_Your_Account_Play_Instantly
References:
Mackie blackjack
References:
https://doc.adminforge.de/s/m0-vm1xrOH
References:
Indiana casino
References:
https://digitaltibetan.win/wiki/Post:Top_US_Live_Online_Casinos_with_Real_Dealers_in_2026
References:
Southern california casinos
References:
https://md.un-hack-bar.de/s/D0P-2Kbb1F
legal anabolic supplement
References:
https://intensedebate.com/people/footpanda97
articles on steroids
References:
https://v.gd/cxFoyU
arnold schwarzenegger use steroid
References:
https://etuitionking.net/forums/users/baboonrhythm8/
monster massive protein review
References:
https://ondashboard.win/story.php?title=d-bal-opiniones-%C2%BFes-el-suplemento-que-realmente-funciona
References:
Fantasy spring casino
References:
https://cameradb.review/wiki/Amt_Mittleres_Nordfriesland_Erlaubnis_beantragen_ein_Glcksspiel_zu_veranstalten_oder_zu_vermitteln
References:
Moncton new brunswick
References:
https://graph.org/Die-besten-Bonus-Angebote-2026-01-29
References:
Online casino u s a
References:
http://king-wifi.win//index.php?title=didriksenherman7852
References:
Video poker para pc
References:
https://www.google.pl/url?q=https://online-spielhallen.de/888casino-mobile-app-ihr-casino-fur-unterwegs/
References:
D casino las vegas
References:
http://pattern-wiki.win/index.php?title=bennettchapman9621
References:
Seminole casino coconut creek
References:
https://lovewiki.faith/wiki/18_Best_Ethereum_Casinos_for_2026
References:
Hollywood casino west virginia
References:
https://pads.zapf.in/s/hLQLNCfaTl
References:
Cosmopolitan casino
References:
https://swaay.com/u/rophercseel55/about/
References:
Casino joe pesci
References:
https://peatix.com/user/28832343
References:
Fiat 500 blackjack
References:
https://www.google.com.uy/url?q=https://blackcoin.co/best-payid-casinos-in-australia-15-sites-that-accept-payid/
References:
Le richelieu in the french quarter
References:
http://dubizzle.ca/index.php?page=user&action=pub_profile&id=129819
where can i get steroids
References:
https://intensedebate.com/people/screenindex92
References:
Steroid alternative gnc
References:
http://jobboard.piasd.org/author/orchidchain84/
best steroid stack to gain muscle
References:
https://hedgedoc.info.uqam.ca/s/jpFURIUBi
what is tren steroid
References:
https://dreevoo.com/profile.php?pid=1057182
References:
Are steroids illegal
References:
https://notes.io/epyiP
bulking cycle steroids
References:
https://sundaynews.info/user/coldnorth57/
steroids detransformation
References:
https://intensedebate.com/people/egyptmist6
References:
Regent casino
References:
https://medibang.com/author/27680111/
References:
Isle capri casino
References:
https://atavi.com/share/xogyowzdyavy
References:
What are the effects of anabolic steroids
References:
https://www.pradaan.org/members/francecicada8/activity/778414/
safe anabolic steroids
References:
http://king-wifi.win//index.php?title=bernardfrandsen8096
References:
Roids uk
References:
https://www.hulkshare.com/gumstock1/
over the counter steroids
References:
http://mozillabd.science/index.php?title=craftcrews8358
References:
Original steroids
References:
https://www.24propertyinspain.com/user/profile/1370456
will one cycle of testosterone hurt you
References:
https://urlscan.io/result/019c2ee8-7fb7-76ea-a4bc-80b7411eeecf/
anabolic steroids online pharmacy reviews
References:
https://korsgaard-mclean-4.thoughtlanes.net/hormone-de-croissance-humaine-hgh-astera-labs-hgh-16iu-injections-a-vendre
maximum shred gnc
References:
http://king-wifi.win//index.php?title=mcclearysilva5011
References:
Legit steroid suppliers
References:
https://pads.jeito.nl/s/pj_cmnLNCi
anabol 10
References:
https://socialisted.org/market/index.php?page=user&action=pub_profile&id=316300
are steroids illegal in usa
References:
http://karayaz.ru/user/masspound15/
do legal steroids work
References:
https://urlscan.io/result/019c325a-16d8-7599-b474-ee6a26c8c390/
what are steroids what are they used for
References:
http://jobs.emiogp.com/author/forkburst3/
References:
Alternative to steroids for bodybuilding
References:
https://doc.adminforge.de/s/xY5M8Bkzzj
References:
Dianabol for beginners
References:
https://md.un-hack-bar.de/s/nxsouFoPOz
drugs for muscle growth
References:
https://wifidb.science/wiki/How_to_Spot_Fake_Anavar_A_Buyers_Survival_Guide
trusted online steroid suppliers
References:
https://swaay.com/u/muirenmgcpq41/about/
anabolic oral steroids
References:
https://urlscan.io/result/019c336c-8d9b-70aa-ba6d-7199a1650279/
References:
Winstrol acne
References:
https://www.blurb.com/user/formcomic8
References:
Tren workout supplement
References:
https://pad.stuve.uni-ulm.de/s/I1jtR9zZJ
lucky casino
References:
https://judgehat22.bravejournal.net/free-100-pokies-no-deposit-sign-up-bonus-australia-in-2025
hard rock casino punta cana
References:
https://www.question2answer.org/qa/user/colonydonna0
planet hollywood casino
References:
https://onlinevetjobs.com/author/shopbucket8/
western lotto max
References:
https://itkvariat.com/user/wealthtoilet2/
canberra casino
References:
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://free100pokiesnodeposit.blackcoin.co
sandia casino albuquerque
References:
https://linkagogo.trade/story.php?title=fair-go-casino-support-24-7-contact-options-for-aussie-players
nouveau brunswick
References:
https://fravito.fr/user/profile/2191464
macau casinos
References:
https://bookmarkzones.trade/story.php?title=mr-o-casino
live casino direct
References:
https://imoodle.win/wiki/Crypto_casino_with_Instant_Withdrawals_and_400_400_Free_Spins_Bonus
casino pier
References:
https://hikvisiondb.webcam/wiki/Galaxy96aus_Reviews_Read_Customer_Service_Reviews_of_galaxy96aus_com
internet casinos
References:
http://ask.mallaky.com/?qa=user/eventpine53
grand casino
References:
http://fprints.com.ua/user/cirrusscene12/
%random_anchor_text%
References:
https://dokuwiki.stream/wiki/Anavar_Erfahrungen_Zyklus_Anavar_Frauen_Steroid_2026
%random_anchor_text%
References:
http://ezproxy.cityu.edu.hk/login?url=https://hcgbeilstein.de/media/com_articles/anavar_kaufen_4.html
dubuque casino
References:
https://tarbiyah.alqolam.ac.id/2022/06/21/jadwal-ujian-proposal-dan-sidang-skripsi-fakultas-tarbiyah-bulan-juni-pekan-ke-iv/
over the counter steriods
References:
https://hedgedoc.eclair.ec-lyon.fr/s/0I8ppdNh7
best steroid for strength and cutting
References:
https://school-of-safety-russia.ru/user/boatsea6/
which is a possible long-term effect of steroid use?
References:
https://erickson-lam.mdwrite.net/buy-clenbuterol-the-best-steroid-source-online
harmful effects of anabolic steroids
References:
https://atavi.com/share/xq4thkz8dqh
References:
Painted hand casino
References:
https://forum.karnex.in/question/cold-chain-packaging-market-drivers-restraints-and-future-opportunities-2032/
References:
Casino holland
References:
https://www.familygreenberg.com/index2.php/2012/01/ch-ch-changes-solution-week-4/
References:
Ameristar casino council bluffs
References:
http://justicefornorthcaucasus.com/jfnc_message_boards/turkey.php?entry_id=1292630032&title=g%C3%9Cnaydin-rusya%21&comments=comments